Asphyxiating thoracic dystrophy (ATD), also known as Jeune syndrome, is an extremely rare chest wall deformity characterized by an abnormally developed thoracic cavity and often involves dysfunction of multiple organs.
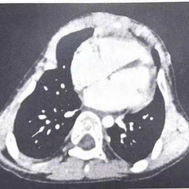
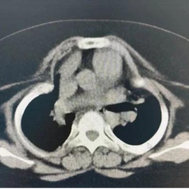
ATD can be classified into two types. Type I ATD is characterized by overall narrowing of the thoracic cage, with both the transverse and anteroposterior diameters markedly reduced compared with a normal chest. Type II ATD is a distinct form of thoracic narrowing, primarily characterized by extensive bilateral depressions of the lateral chest walls. The depressions involve multiple ribs and often extend to the costal arches.
The constriction of the chest severely impairs respiratory function, making ATD a critical condition. Most patients succumb to hypoxia soon after birth.