Even after a successful chest wall surgery, proper wound healing remains a key concern. If a wound doesn’t heal as expected, it can cause pain, slow recovery, and in some cases lead to infection, potentially affecting the overall results of the surgery. Understanding why healing problems occur and how to address them is essential for a safe and timely recovery.
1. Causes
Poor wound healing usually means delayed healing, exudation, dehiscence, or infection. If an incision fails to heal for a prolonged period, it is prone to developing into an infection. Incision infection usually results from the combined effects of bacterial invasion and compromised host resistance—Intraoperative or postoperative handling can provide an opportunity for bacteria to invade, while conditions such as anemia, poor nutrition, or chronic debilitating conditions can make infections more likely.
Other factors that can affect wound healing include the blood supply at the incision site, the method of plate fixation, the suturing technique, and the appropriate use of antibiotics. In most cases, incision infection arises from multiple contributing factors.
2. Symptoms
Incision infections can present with local or systemic symptoms, and their severity varies widely among patients. Since most chest wall surgery incisions are small, early infections are usually limited to the area around the incision. In the early stage, the incision may appear red and swollen, with the skin feeling warm and slightly painful.
As the infection worsens, an abscess may form at the incision site, causing stronger pain. When the abscess enlarges, it may rupture, temporarily easing the pain, but pus may continue to drain from the wound. Persistent infections may lead to the formation of small channels within the wound (medically called sinus tracts or fistulas), through which pus continuously flows out. In severe cases, the bar may even become exposed.
In some cases, the infection can spread to the chest cavity or the rest of the body, causing high fever, chills, widespread pain, and even impaired breathing. In extremely rare and severe cases, patients may develop septic shock, which can be life-threatening.
3. Treatment
After an incision infection occurs, treatment—either conservative or surgical—can be chosen based on the severity of the infection.

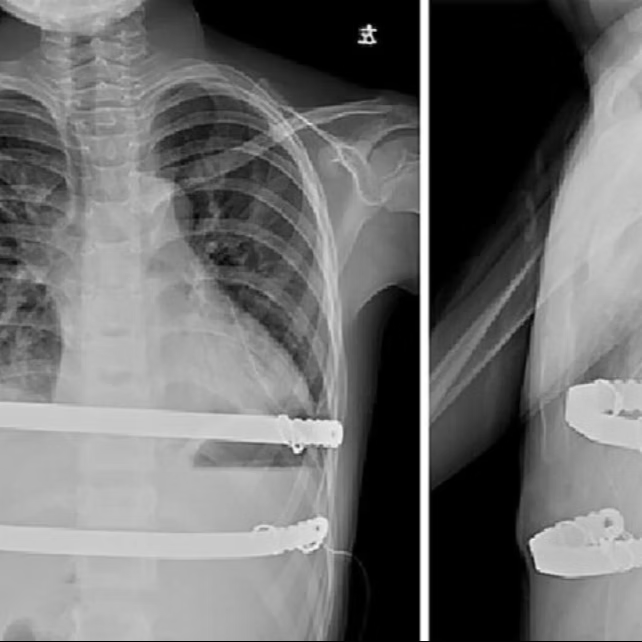
before and after surgery
a. Conservative management
In conservative treatment, antibiotics are first used to control the infection. For early or mild infections, physical therapies such as warm compresses or infrared therapy can also be applied to help reduce inflammation and promote recovery.
If an abscess has formed in the incision, or if incision dehiscence occurs with persistent purulent drainage, local debridement is required to remove the pus and any necrotic tissue, followed by the placement of a drainage tube. Smaller wounds may gradually heal with regular dressing changes after debridement. For slower-healing or more severe infections, some patients may receive negative wound pressure therapy, in which a dressing and drainage tube are applied to the wound and connected to a vacuum device. The gentle, steady suction helps remove excess pus, keep the wound clean, and promote healing. Treatment for incision infections often takes time, and patients are advised to remain patient and actively follow their treatment plan.
b. Surgical treatment
If the infected incision fails to heal after conservative treatment, surgical intervention may be required.
During surgery, the infected region and any necrotic tissue within the incision are first thoroughly removed. In some cases, the incision is extended slightly to ensure complete debridement. Sutures in the infected area are then carefully removed. Since the implanted bar provides essential structural support and plays a key corrective role, it is typically left in place.
In addition, any residual cavity inside the incision is addressed during the procedure. A residual cavity is a gap where the skin has not fully adhered to deeper tissues such as muscle or fascia, or a space created after infected or necrotic tissue has been removed. If fluid accumulates in these spaces, the wound can become a breeding ground for bacteria, hindering the healing process. After surgery, drainage tubes are commonly placed to drain excess fluid, prevent further buildup, and thereby lower the risk of infection.
When the incision is closed, a special suturing technique called tension-reducing suturing may be applied for relatively small areas of tissue damage. This method distributes tension across the skin, reducing the risk of the incision reopening and protecting the blood supply. For larger defects, tissue flaps can be used, in which healthy tissue from another part of the body covers the defects to promote proper healing.
Whether an incision heals properly depends not only on the surgical operation but also on the patient's postoperative cooperation. Bathing too soon after surgery, repeatedly rubbing or bumping the incision, removing dressings without authorization, or exposing the incision to contaminants can all increase the risk of infection. Therefore, during recovery from chest wall correction surgery, patients should strictly follow their doctor’s instructions for wound care, change dressings on schedule, avoid inappropriate activities, and seek medical attention promptly if abnormalities such as redness, worsening pain, or discharge occur.

before surgery

The first-stage debridement and negative wound pressure therapy

after surgery