Pectus carinatum, also known as “pigeon chest”, is a chest wall deformity characterized by a protrusion of the sternum and connecting costal cartilages. While often considered primarily a cosmetic issue, this condition can cause significant psychological distress and, in some cases, mild physical limitations. For patients seeking definitive, long-term correction, the question of how to fix pectus carinatum leads them to explore specialized pectus carinatum surgeries.
This guide offers a clear look into the diagnostic process and a detailed overview of the primary surgical options designed to effectively correct this deformity.
Understanding Pectus Carinatum (Pigeon Chest)
Pectus carinatum is a chest wall deformity characterized by a protrusion of the sternum and ribs (usually 3–7 ribs). The protrusion can assume various morphologies, including a ridge, hull, peak, or spherical mass, and may be accompanied by depressions in the lateral and lower chest wall. It is sometimes referred to as “pigeon breast” due to its distinctive appearance.

severe pectus carinatum
Prevalence
Pectus carinatum deformity affects approximately 1 in 1,000 people, though some estimates suggest it may be as common as 1 in 300. It is more prevalent in males than females and is typically most noticeable during adolescent growth spurts.
Causes
Currently, the exact cause of pectus carinatum remains unclear. It may involve multiple factors, such as congenital developmental abnormalities, genetic factors (up to 33% of patients have a family history of chest wall abnormalities), nutritional influences, and certain diseases, such as chronic respiratory infection and chest wall tumors. In some cases, pectus carinatum may manifest as a complication after cardiac surgery.
Symptoms
Most patients do not exhibit noticeable symptoms. However, patients with severe deformities may present with mild chest discomfort, shortness of breath, or fatigue. Additionally, some patients may frequently suffer from asthma or upper respiratory infections, leading to reduced physical endurance and easy fatigue.
It is worth noting that chest wall deformities often cause a psychological burden for patients. Some individuals develop low self-esteem, social anxiety, or tend to avoid sports and activities that expose the chest. These psychological issues can sometimes contribute to physical discomfort, such as chest tightness and chest pain.
Gain deeper insight into:
Can patients with pectus carinatum (PC) have difficulty breathing?
Pectus Excavatum vs. Pectus Carinatum: Key Differences
Diagnosis and Evaluation of Pectus Carinatum
Diagnosis
Pectus carinatum can be diagnosed through physical examination and imaging studies.
-
The doctor will conduct a comprehensive physical examination and obtain a detailed medical history to assess the patient's signs and symptoms.
-
Further diagnostic evaluations, such as an electrocardiogram (ECG) and X-ray, are needed. A CT scan is further indicated when other conditions are suspected.
- During diagnosis, it is important to differentiate pectus carinatum from other conditions such as Wenlin chest, Poland syndrome, complex chest wall deformities, saddle chest, and asphyxiating thoracic dysplasia.
When is Pectus Carinatum Surgery Recommended?
For young children with mild deformities, early surgical intervention is not recommended, and non-surgical approaches may be considered instead.
The primary method is the use of orthotic bracing. This involves wearing a custom-made external brace that applies continuous, targeted pressure to the protruding area, gradually reshaping the chest wall contour. Sometimes professional physical therapy and functional training are used as supplementary methods to improve posture and muscle strength, but they cannot correct the underlying skeletal abnormality.
Surgical Indications
Pectus carinatum surgery should be prioritized when the following conditions are present:
1. Severe or significantly asymmetrical pectus carinatum deformities
2. Pectus carinatum resulting from cardiac surgery
3. The patient desires a permanent pectus carinatum repair
4. Poor compliance with or ineffectiveness of bracing therapy
5. The deformity causes severe psychological distress and body image issues
A Closer Look at 3 Pectus Carinatum Surgical Procedures
The surgery for pigeon chest varies significantly in technique, ranging from open surgery to minimally invasive methods using steel bars. Choosing the appropriate surgical procedure for pectus carinatum largely depends on the individual’s anatomical structure and the severity of the deformity.
The following discusses 3 common surgeries for pectus carinatum:
|
Procedure |
Nature of Surgery |
Surgical Operation Overview |
Advantages
|
Challenges |
|
Ravitch Procedure |
Open, Invasive |
A midline incision is made to resect costal cartilage; in some patients with a prominent sternum, a sternal osteotomy is required. |
Effective for severe and complex cases of pectus carinatum. |
Highly invasive, long recovery period, and potential for significant scarring. |
|
Abramson Procedure |
Minimally Invasive |
The shaping bars are placed on the surface of the protruding bony structure of the chest wall, and manual pressure is applied to push the protruding chest wall downward. Finally, fixation bars are used to fix both ends of the shaping bars to the ribs. |
Minimally invasive, less trauma, faster recovery, and smaller scars. |
Limited indications; lateral bar fixation remains a challenge in the Abramson procedure. |
|
Wenlin Procedure |
Minimally Invasive |
The shaping bars are placed on the protruding chest wall, and steel wires pull the bone structures on both sides outward until the protrusion disappears and the chest wall contour aligns with the bars. Finally, the wires secure both ends of the bars to the ribs. |
Less trauma, faster recovery, more ideal outcomes, and greater safety. Applicable to various protrusive deformities, with no age or other restrictions. |
Requires an experienced surgical team. |
1. Ravitch Procedure (Open or Modified)
The Ravitch procedure, developed in the mid-20th century, is a classic open method for correcting chest wall deformities. It is considered the standard for severe or complex pectus carinatum surgery. The operation involves a midline incision over the sternum, cartilage resection, and an osteotomy.
Its corrective effect is thorough and long-lasting.
The drawbacks are that it is more invasive, leaves a longer incision, and has a longer recovery period compared to minimally invasive procedures.
2. Abramson Procedure
The Abramson procedure is a minimally invasive method that emerged in the early 21st century, inspired by the Nuss procedure (used for pectus excavatum repair). This pectus carinatum surgery involves making two incisions, approximately 3–4 cm in length, on either side of the chest. These incisions are used to place curved shaping bars subcutaneously in front of the sternum, applying inward pressure to the protruding area. Finally, the two ends of the bars are fixed to the ribs using short fixation bars. The bars are typically retained for about 2–3 years.
Compared to open surgery, this surgery for pectus carinatum features smaller incisions, is less traumatic, and has a faster recovery.
However, this technique only enables an overall correction of the protrusion and cannot precisely address localized deformities. This prevents the chest wall contour from perfectly matching the shaped bars, leading to suboptimal correction. In addition, because the short fixation bars are relatively bulky, their use may necessitate a longer incision and potentially interfere with proper wound healing. In severe cases, this can result in complications such as bar displacement, incision breakdown, infection, and pus discharge.
Additionally, the Abramson procedure is not suitable for older patients or those with very severe deformities, such as pectus carinatum with acute angle deformity.
3. Wenlin Procedure
The Wenlin procedure is an innovative minimally invasive pectus carinatum surgery developed by Dr. Wenlin Wang. It is primarily intended for the treatment of pectus carinatum, but is also applicable to other convex deformities, such as costal arch protrusion or complex chest wall deformities with protrusion. This pectus carinatum surgery has no age or other specific restrictions for patients.
It employs special techniques such as "Pre-shaping" and the "Wang Technique," which effectively overcome some of the drawbacks and risks of the Abramson procedure, making it applicable to older patients or those with severe pectus carinatum.
- Pre-shaping Technique
It involves using instruments to lift or compress the deformed chest wall, or resecting part of the deformed bones. This makes the chest wall skeleton more flexible and easier to shape, ensuring a smoother subsequent correction with steel bars. Therefore, this technique is particularly suitable for patients with severe deformities or those of advanced age.
- Wang Technique
It replaces the use of short fixation bars by directly securing the two ends of the shaping bars with steel wires. This fixation method simplifies the operation and enhances stability, thus significantly reducing the risk of bar displacement, poor incision healing, and other complications.
Learn in detail: Pre-shaping: revolutionizing the treatment of severe and complex chest wall deformities

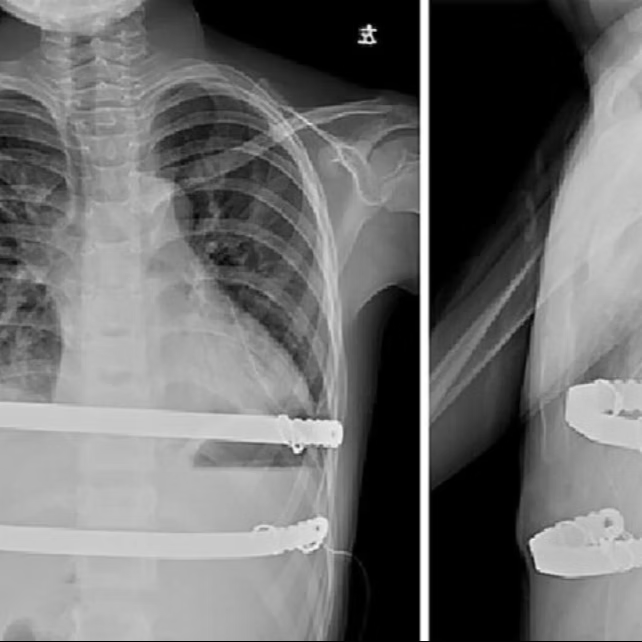
Surgical technique of the Wenlin procedure 
Pre- and postoperative chest X-rays
Ultimately, the choice of pectus carinatum surgery should be determined by multiple factors, including the severity of the deformity, the patient’s age, chest wall structure flexibility, as well as individual needs and expectations. It is crucial for patients to consult experienced specialists to receive a personalized diagnosis and treatment plan, helping them fully overcome the challenges caused by pectus carinatum deformity.
The Expert Team at ICWS
ICWS is the world’s largest chest wall deformity correction center, led by Dr. Wenlin Wang. The team has pioneered numerous surgical techniques globally, including the Wenlin procedure. The ICWS expert team has extensive experience in managing a wide spectrum of pectus carinatum cases, ranging from mild to extremely severe, and emphasizes precision and patient-centered care in treatment. They have successfully carried out more than 10,000 chest wall surgeries for patients worldwide.
ICWS remains dedicated to providing safe and effective treatment options for patients with pectus carinatum and other chest wall deformities, helping them regain health and confidence.