In this article, we will introduce six common types of chest wall deformities and provide a brief exploration of their diagnostic methods and treatment options.
What is Chest Wall Deformity?
Chest wall deformity is a condition characterized by an abnormal shape or development of the sternum, ribs, and costal cartilages.
Common symptoms often include noticeable changes in chest shape, such as a sunken sternum (pectus excavatum) or a protruding chest (pectus carinatum). Some individuals may also experience shortness of breath, chest tightness, or palpitations, and in severe cases, heart and lung function may be affected.
These different types of chest wall deformity can cause psychological distress and social anxiety for many patients. For children and adolescents, the associated psychological burden may be more severe and long-lasting.
Additionally, chest wall deformities can worsen with age, leading to increasingly noticeable symptoms and discomfort. Therefore, early diagnosis and timely surgical correction are generally recommended.
The Six Most Common Types of Chest Wall Deformities
Among different types of chest wall deformities, the two most common are Pectus Excavatum and Pectus Carinatum, which together account for the majority of cases.
Below, we explore 6 common types of chest wall deformities:
1. Pectus Excavatum (sunken chest or funnel chest)

Pectus Excavatum, also called Sunken Chest or Funnel Chest, is the most common chest wall deformity, characterized by a depression of the breastbone.
According to a 2024 review published in the Journal of Thoracic Disease, Pectus Excavatum accounts for approximately 65–95% of all chest wall deformities, with an incidence of up to 8 per 1,000 live births[1]. The male-to-female ratio is reported to range between 3:1 and 5:1[1,2].
However, due to the lack of large-scale global studies and inconsistent diagnostic criteria, the true prevalence of Pectus Excavatum may be underestimated.
- Main Characteristics: The breastbone is depressed inward, forming a funnel-shaped chest.
- Cause: The exact cause remains unclear. It may be related to abnormal development of the ribs and costal cartilages, genetic factors, or connective tissue disorders.
- Effect: Mild cases typically cause no significant symptoms, while moderate to severe cases may affect cardiopulmonary function, causing symptoms such as palpitations, shortness of breath, and even breathing difficulty.
Find out more about the common questions and major types of pectus excavatum.
2. Pectus Carinatum (pigeon chest)

Pectus Carinatum, also known as Pigeon Chest, is the second most common type of chest wall deformity. It is characterized by a protrusion of the sternum, resulting in a visibly convex chest appearance.
This type of chest wall deformity is reported to occur 2 to 4 times less frequently than pectus excavatum, and its incidence in males is estimated to be about four times higher than in females[1].
- Main Characteristics: The sternum and ribs protrude in such a way that the chest may appear ridge-like, hull-shaped, peaked, or rounded. Depressions may also appear on the lateral or lower chest walls.
- Causes: The exact cause of pectus carinatum remains unclear. It may be associated with genetic factors or calcium deficiency. Secondary pectus carinatum is commonly observed in young children following cardiac surgery.
- Effects: The visible protrusion can cause cosmetic and psychological concerns, and in severe cases may affect respiratory and circulatory function. Moreover, children may exhibit impaired growthand recurrent respiratory infections.
Read more: Pectus Excavatum vs. Pectus Carinatum: Key Differences
3. Barrel Chest

Barrel Chest is a type of chest wall deformity that gives the thorax a round, barrel-like appearance. It is most commonly seen in patients with advanced emphysema[3,4], and may also arise from thoracic, pleural, and cardiovascular diseases, as well as some other factors.
- Main Characteristics: The overall thoracic shape appears barrel-like, with the increased anteroposterior diameter that is nearly equal to the transverse(left-right) diameter.
- Causes: It can be primary (congenital) or secondary to intrathoracic or systemic diseases. Among them, chronic respiratory diseases such as emphysema are the most common causes of secondary barrel chest.
- Effects: Patients with primary barrel chest usually have no obvious symptoms, while those with secondary barrel chest often experience respiratory symptoms due to underlying diseases, such as cough, chest pain, dyspnea, shortness of breath, or hemoptysis.
Find out more about What Causes A Barrel Chest?
4. Flat Chest
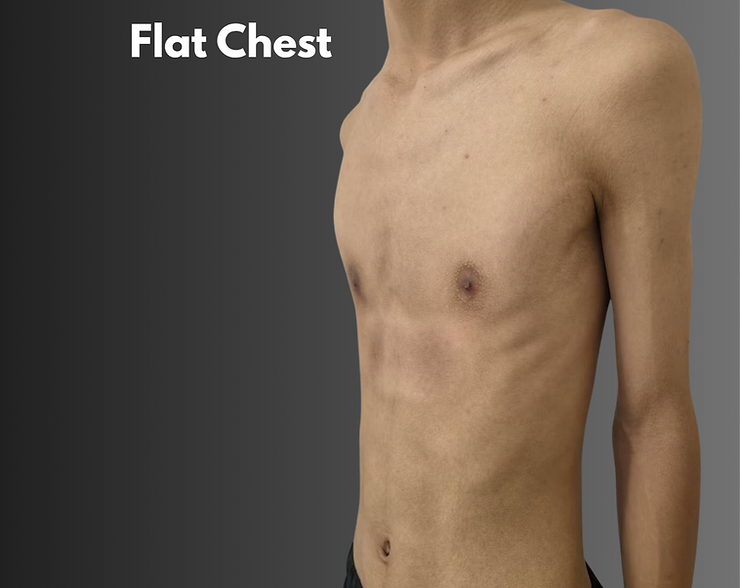
Flat Chest is clinically defined by a markedly reduced anteroposterior diameter of the thoracic cage—less than half of its transverse diameter—resulting in a visibly flattened chest appearance.
- Main Characteristics: The entire chest wall is sunken, presenting a visibly flattened shape.
- Causes: The exact cause remains uncertain. It may be associated with genetic factors
,or result from malnutrition, chest trauma, systemic wasting diseases, or pulmonary conditions. - Effects: Flat chest may compress the heart and lungs, causing palpitations, chest tightness, and shortness of breath. It can also cause serious psychological stress and mental health problems. Additionally, patients with flat chests are more prone to spontaneous pneumothorax.
Find out more about What do people with flat chest deformity feel like?
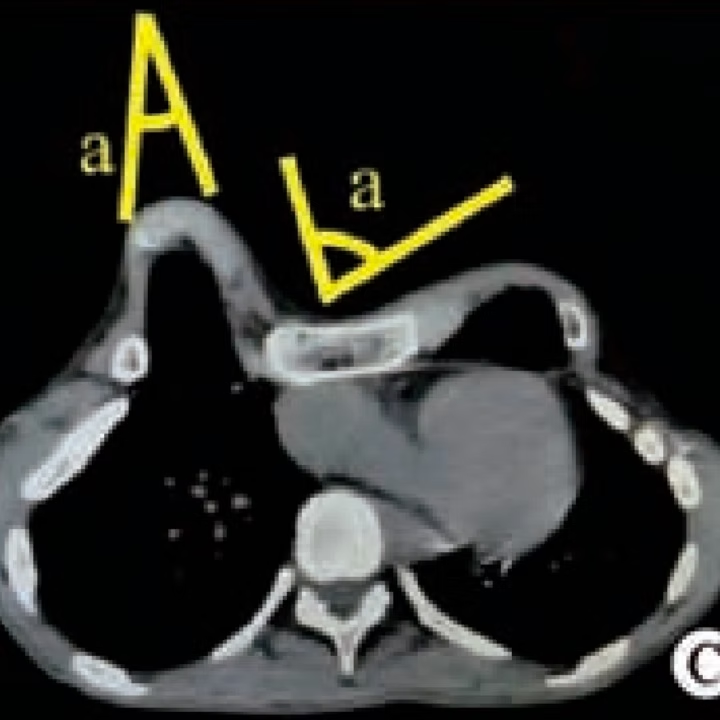
5. Costal Arch Deformity

Costal Arch Deformity refers to structural abnormalities of the costal arch , which typically manifest as localized protrusion or depression. This deformity may occur independently or in combination with other types of chest wall deformity.
- Main Characteristics: Protrusion of the costal arch is most common, while depression or mixed deformities are less frequent.
- Causes: The cause of primary costal arch protrusion remains unknown. Secondary costal arch deformities are most often observed in adults after pectus excavatum surgery and in young children with severely protruding abdomens.
- Effects: In some cases, the deformity is cosmetically noticeable and may negatively affect psychological well-being.
6. Complex Chest Wall Deformity

(A) and (B) appearance of the chest wall before operation, (C) feet and (D) hands[5].
This type of chest wall deformity features both protrusions and depressions on the anterior chest wall.
- Main Characteristics: The appearance and shape of the convexities and concavities vary widely among individuals, exhibiting diverse and complex forms.
(*Note: Some conditions — such as saddle chest, grooved chest, Wenlin chest, and Poland syndrome — may also exhibit both depressions and protrusions. However, due to their distinct and fixed morphological characteristics, they are not classified as complex chest wall deformities.)
- Effects: The abnormal appearance of the chest wall frequently leads to self-consciousness and reduced self-esteem. In cases where the depressed regions compress the heart and lungs, patients may experience cardiopulmonary symptoms similar to those observed in pectus excavatum.
ICWS is the world’s first independent surgical treatment institution specializing in chest wall disorders and the largest chest wall deformity correction center globally.
At ICWS, our expert team utilizes personalized, minimally invasive techniques to achieve precise correction for a wide spectrum of chest wall deformities.
How Are Chest Wall Deformities Diagnosed?
Diagnosis of chest wall deformity is made through physical examination, imaging studies, and functional tests. The following tests are typically performed:
- Physical Examination: to check the appearance, severity, and movement of the chest wall.
- Cardiac assessment: such as electrocardiogram (ECG) and echocardiography.
- Pulmonary function assessment: such as pulmonary function test and arterial blood gas analysis.
- Deformity assessment: such as X-ray, chest CT, and 3D modeling.
These tests aid in the evaluation of deformity severity and the optimal chest wall deformity treatments for every patient.
Chest Wall Deformity Treatments
Both surgical and non-surgical treatments are available, depending on the patient’s age, type of deformity, and its severity.
Non-Surgical Treatments
- Bracing Therapy – utilized most often in cases of mild Pectus Carinatum, particularly in teenagers.
- Physical Therapy and Breathing Exercises – improving posture, muscle strengthening, and optimal chest expansion.
- Vacuum Bell Therapy – primarily used for mild Pectus Excavatum, using suction to slowly draw the chest wall outwards.
Surgical Treatments
For patients with different types of chest wall deformity, ICWS offers a variety of innovative surgical techniques.
These corrective surgeries are less invasive, lower risk, and deliver better outcomes compared to traditional techniques such as the classic Nuss procedure and the Abramson procedure.
1. Wang Procedure
Indications: Pectus Excavatum, Poland Syndrome, Flat Chest, Saddle Chest, Wenlin Chest
Pioneered by Dr. Wenlin Wang, this procedure’s greatest advantage lies in its ability to correct deformities while avoiding injury to the heart and lungs—one of the main risks with the classic Nuss procedure, a mainstream surgical technique for treating pectus excavatum.
The Wang Procedure can be safely performed on children under five years old (the youngest successfully treated patient was only one month old) without interfering with normal skeletal development.
In 2019, the Wang Procedure received official recognition from the National Health Commission of China and became one of the standard surgical techniques for treating pectus excavatum in China.
Further reading:
3 Minimally Invasive Surgeries for Pectus Excavatum
What are the differences between the Wang procedure and the Nuss procedure?
What special types of pectus excavatum(PE) are suitable for the Wang procedure?
2. Wung Procedure
Indications: The indications for the Wung Procedure are the same as those for the Wang Procedure. The two techniques can be flexibly selected and applied based on individual clinical conditions.
The Wung Procedure is a modified surgical technique developed from the standard Nuss procedure. It effectively addresses common challenges and risks of the Nuss procedure, such as potential heart injury during bar placement and instability of bar fixation. These innovations not only simplify the surgical process but also significantly reduce operative difficulty and associated risks.
Further reading: The differences between the Wung procedure and the Nuss procedure
3. Wenlin Procedure
Indications: Pectus Carinatum, Costal Arch Convex Deformity, Wenlin Chest, Flat Pectus Carinatum, Barrel Chest
The Wenlin Procedure, developed by Dr. Wenlin Wang, is an innovative minimally invasive surgical technique specifically designed for the correction of Pectus Carinatum. Compared with the classic Abramson procedure, the Wenlin Procedure differs in surgical details and incorporates innovative concepts and techniques, such as the “Pre-shaping” concept and the “Wang Technique.”
This approach provides more effective correction of protruding deformities, with advantages including minimal trauma, superior cosmetic results, improved safety and simplicity, shorter recovery time, and lower complication rates.
Further reading: Pre-shaping: revolutionizing the treatment of severe and complex chest wall deformities
Correction of Complex Chest Wall Deformities:
For Complex Chest Wall Deformities, where both protrusion and depression commonly coexist in most cases, a combination of these procedures is flexibly applied to achieve simultaneous correction.
Furthermore, for some severe cases, chest wall reconstruction surgery may also be needed.
Contact ICWS for Chest Wall Correction Surgery
If you or your family member is suffering from a chest wall deformity, we invite you to make an evaluation appointment at ICWS. For further information regarding our procedures, patients’ journeys, and recovery results, visit our official website or contact us now.
References:
[1] Janssen N, Daemen JHT, Franssen AJPM, et al. Pectus excavatum and carinatum: a narrative review of epidemiology, etiopathogenesis, clinical features, and classification. J Thorac Dis. 2023;15(10):4120–4139. Available at: https://jtd.amegroups.org/article/view/82552/html.
[2] Biavati M, Kozlitina J, Alder AC, et al. Prevalence of pectus excavatum in an adult population-based cohort estimated from radiographic indices of chest wall shape. PLoS One. 2020;15(5):e0232575. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC7205298/.
[3] Zafar MA, Patil GA, Maheshwari A, et al. Physical signs in patients with chronic obstructive pulmonary disease. Lung India. 2019;36(1):45–52. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6330798/.
[4] Park KJ, Park SY, Lee SH, et al. Altered thoracic cage dimensions in patients with chronic obstructive pulmonary disease. Respir Res. 2018;19(1):54. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC5874141/.
[5] Wenlin C, Wung C, Wenhao H, et al. Minimally invasive operation of severe complex thoracic deformity with Wenlin procedure and Wung procedure. J Surg Case Rep. 2022;2022(10):rjac473. Available at: https://academic.oup.com/jscr/article/2022/10/rjac473/6772486.