Asphyxiating thoracic dystrophy, commonly known as Jeune syndrome, is a rare and potentially life-threatening thoracic deformity. This article offers a systematic overview of its definition, classification, etiology, clinical manifestations, diagnostic approaches, and current surgical treatment strategies.
Asphyxiating Thoracic Dystrophy (Jeune Syndrome)
Asphyxiating thoracic dystrophy (ATD) is a rare autosomal recessive disorder[1,2]with an estimated prevalence of 1 in 100,000 to 150,000 live births[3,4].
The typical features of this disorder are abnormalities in the structure and shape of the thoracic cage. Systemic skeletal, renal, and gastrointestinal involvement may also be present.
The most critical threat of ATD lies in the narrowing of the thoracic cage, which restricts lung development and may result in severe respiratory distress immediately after birth. Failure to address these respiratory challenges early can result in high neonatal mortality. Therefore, ATD is a highly life-threatening disorder that requires early surgical intervention to increase thoracic cavity volume and alleviate pulmonary compression.
Classifications: Type I vs. Type II ATD
ATD primarily manifests as narrowing of the thoracic cage and can therefore be classified into two types:
1. Type I: Manifests as generalized constriction of the thoracic cage. Both the transverse and anteroposterior (AP) diameters are significantly smaller than those of a normal chest.
2. Type II: A special form of thoracic narrowing, mainly featuring extensive depressions at the costochondral junctions on both sides of the chest wall. These depressions result from abnormal growth direction of the costal cartilages and ribs, involving multiple ribs along the lateral chest wall and often extending to the costal arches.
Distinct differences are also observable in clinical signs:
-
Type I patients: The thoracic cage presents a cylindrical appearance with global constriction and an approximately circular transverse cross-section.
-
Type II patients: The thoracic cage exhibits a midline anterior protrusion with bilateral concavities, resulting in an overall narrowed morphology.

Causes of Asphyxiating Thoracic Dystrophy
In studying the etiology of ATD, it is necessary to distinguish between two concepts: primary ATD and secondary ATD.
1. Primary ATD
The pathogenesis of primary ATD remains unclear. Current research suggests that it may be related to genetic factors, gene mutations, or abnormal growth directions of the ribs and costal cartilages.
(In certain families affected by ATD, mutations in several different genes have been identified as potentially causative, such as DYNC2H1[5,6] and IFT80[7]).
2. Secondary ATD
Secondary ATD refers to thoracic narrowing that arises not from congenital factors but as a complication of previous surgical interventions for thoracic deformities. Typically, such patients have a history of open surgical procedures during which the costal cartilages were excised. Postoperatively, due to the inability of the residual bone structures to regenerate, narrowing of the thoracic cage develops.
Secondary ATD is relatively uncommon in current clinical practice. However, it is important to note that these patients have undergone previous surgeries, which often leads to adhesions and makes reoperation more challenging.
Symptoms and Risk of Asphyxiating Thoracic Dystrophy
While a restricted chest is the most visible sign, asphyxiating thoracic dystrophy actually leads to pathologies in multiple organs throughout the body and manifests various clinical symptoms.
Symptoms of ATD
Common manifestations include thoracic narrowing, dyspnea, and recurrent respiratory infections. As the disease progresses, patients may also present with renal, hepatic, and retinal disorders[8].
In addition, patients with this disorder are typically of short stature and exhibit disproportionate limb development, with some individuals presenting with polydactyly (extra fingers or toes).
Impacts and Consequences
Based on the aforementioned symptoms, the impacts of ATD can be categorized into two primary dimensions:
First, there is the impact on the overall shape and appearance of the chest. Pronounced physical deformities often impose a significant psychosocial burden on patients.
Second, ATD significantly influences physiological function.
Thoracic abnormalities directly impair respiratory function and, if not effectively treated, can lead to death in early life. Beyond respiratory involvement, patients may exhibit lesions in multiple organs, which can affect organ function in various ways.
Diagnosis of Asphyxiating Thoracic Dystrophy
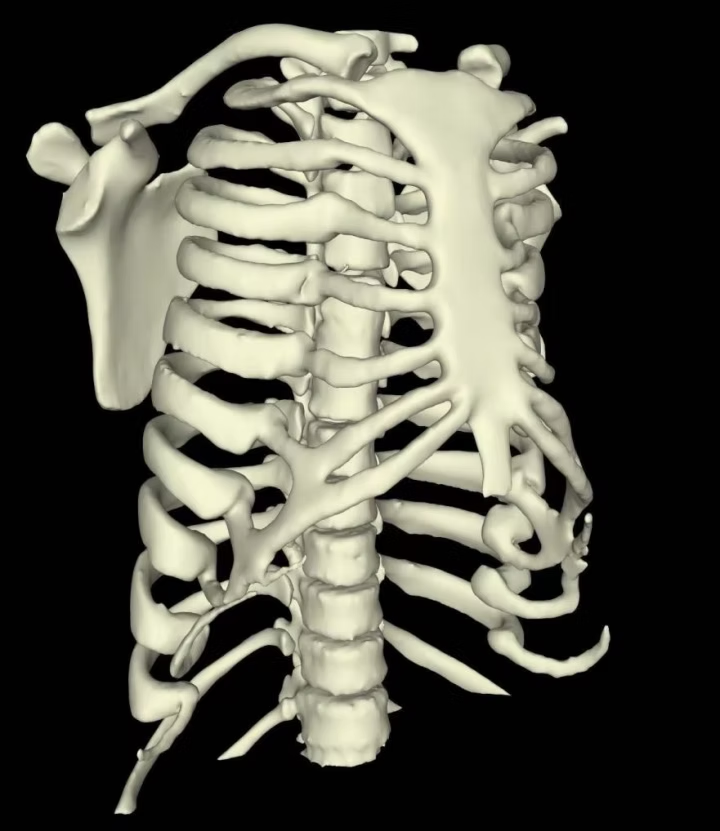
Physical examination can provide a preliminary diagnosis of ATD, while detailed structural information must be obtained through imaging studies.
Common imaging studies include X-ray, chest CT scan, and 3D reconstruction.
Surgical Treatment of Asphyxiating Thoracic Dystrophy
The major risk of ATD lies in compression of the lungs, which results from narrowing of the thoracic cage. To relieve this compression, the thoracic cage must be expanded, and surgery (also known as Jeune syndrome surgery) is the only effective option.
1. For Type I ATD — Chest Wall Expansion Surgery
Median Sternotomy Expansion: A midline incision is made to incise the sternum, followed by the use of MatrixRIB plates to spread the sternum apart, thereby expanding thoracic capacity.
Lateral Thoracic Expansion: Ribs on both sides are cut from the midline and connected using MatrixRIB plates to increase thoracic volume.
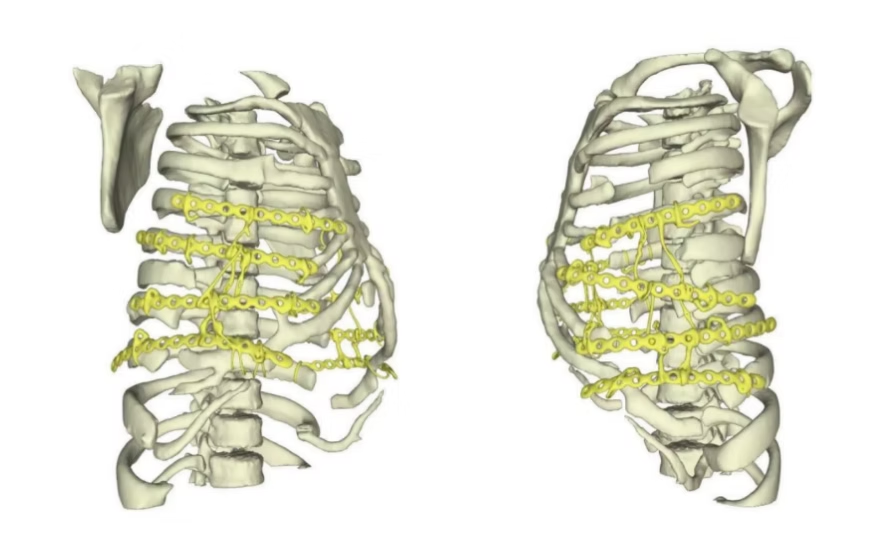
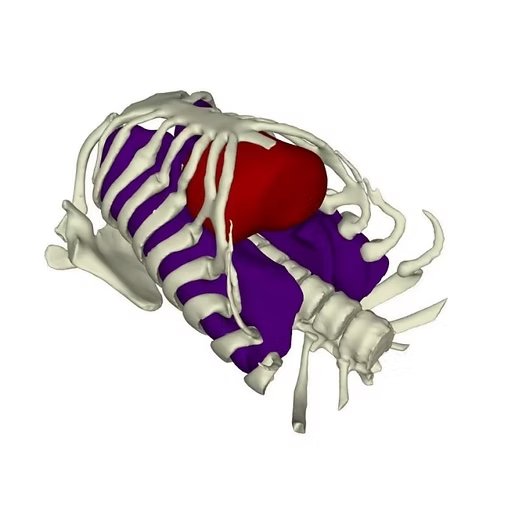
2. For Type II ATD — Wenlin procedure & Wang procedure
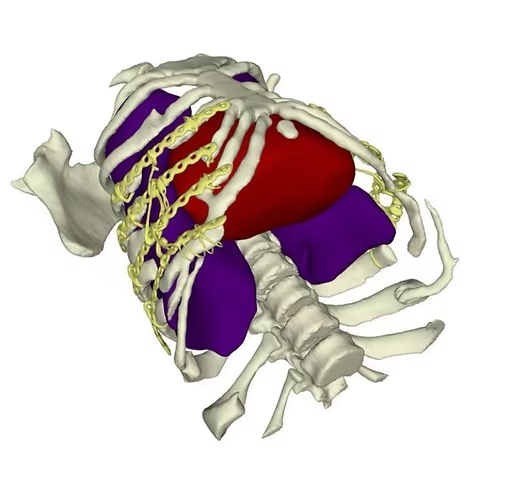
Most Type II ATD patients have both anterior chest wall protrusion and lateral chest wall depressions, so the Wenlin procedure is performed first—using two pre-shaped bars for the operation, with the central part of the bars compressing the anterior protrusion; at the same time, steel wires are used to pull the depressed ribs and costal cartilages on both sides. As shown in the figure:
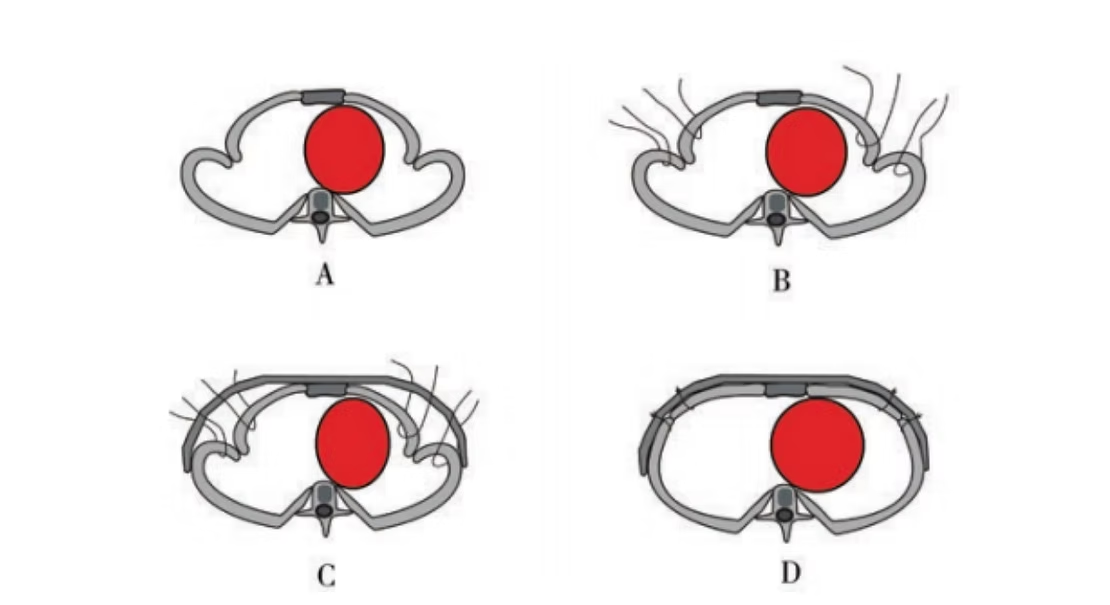
At the same time, due to the large extent of the depressions, the Wang procedure is further used to correct the residual depressions in the lower lateral chest wall, thereby eliminating all deformities and restoring normal chest wall shape.
In addition, for the minority of Type II patients with only lateral chest wall depression deformities, the Wang procedure alone can be used for treatment — pulling the depressions on both sides of the chest wall, and finally using steel wires to securely fix the ribs and costal cartilages to the MatrixRIB bar.
These surgical techniques were developed by ICWS, the world's first independent chest wall disorder surgical treatment institution and the world's largest chest wall deformity correction center. Led by Dr. Wenlin Wang, ICWS has pioneered multiple innovative surgical techniques that effectively address complex and rare chest wall deformities in diverse patient populations.
ABOUT ICWS: The Institute of Chest Wall Surgery
Further Professional Reading: What are the differences between the Wang procedure and the Nuss procedure?
Frequently Asked Questions for Patients and Families
1. Is Asphyxiating Thoracic Dystrophy (Jeune Syndrome) a hereditary disease?
Yes, it is an autosomal recessive condition.
2. Can Jeune Syndrome be cured?
ATD, also known as Jeune syndrome, is an extremely rare and complex thoracic deformity that currently has no definitive cure. At present, treatment options are limited to surgical intervention, which primarily focuses on expanding thoracic volume to significantly improve respiratory function and enhance physical appearance.
3. Can Jeune Syndrome be detected before birth?
Yes. The condition can be detected during the fetal period through prenatal ultrasound imaging[9]. However, it is more commonly diagnosed after birth via X-rays. Genetic testing can also be used to assist in the diagnosis of Jeune Syndrome.
4. What should parents do if their child has Jeune Syndrome?
Time is of the essence. Please schedule a consultation as soon as possible via the ICWS contact page or email. Experts at ICWS will review the case, provide a comprehensive evaluation, and develop a personalized surgical plan. Email: info@icwsorg.com.
5. Are there cases of adults with Jeune Syndrome?
Yes. There are documented cases of adults living with Jeune Syndrome[10]. In some milder cases, or through various medical interventions, some patients are able to survive into adulthood. However, they may still face complications related to respiratory failure or renal and hepatic involvement.
References:
[1] Phillips, J. D., & Van Aalst, J. A. (2008). Jeune’s syndrome (asphyxiating thoracic dystrophy): congenital and acquired. Seminars in Pediatric Surgery, 17(3), 167–172. https://doi.org/10.1053/j.sempedsurg.2008.03.006
[2] Wang, W., Long, W., Liu, Y., Cai, B., & Luo, J. (2022). Surgical treatment of an overgrown asphyxiating thoracic dystrophy patient. Journal of Surgical Case Reports, 2022(11). https://doi.org/10.1093/jscr/rjac530
[3] Oberklaid, F., Danks, D. M., Mayne, V., & Campbell, P. (1977b). Asphyxiating thoracic dysplasia. Clinical, radiological, and pathological information on 10 patients. Archives of Disease in Childhood, 52(10), 758–765. https://doi.org/10.1136/adc.52.10.758
[4] Phillips, J. D., & Van Aalst, J. A. (2008b). Jeune’s syndrome (asphyxiating thoracic dystrophy): congenital and acquired. Seminars in Pediatric Surgery, 17(3), 167–172. https://doi.org/10.1053/j.sempedsurg.2008.03.006
[5] Dagoneau, N., Goulet, M., Geneviève, D., Sznajer, Y., Martinovic, J., Smithson, S., Huber, C., Baujat, G., Flori, E., Tecco, L., Cavalcanti, D., Delezoide, A., Serre, V., Merrer, M. L., Munnich, A., & Cormier-Daire, V. (2009). DYNC2H1 mutations cause asphyxiating thoracic dystrophy and short Rib-Polydactyly syndrome, type III. The American Journal of Human Genetics, 84(5), 706–711. https://doi.org/10.1016/j.ajhg.2009.04.016
[6] National Organization for Rare Disorders (NORD): Asphyxiating Thoracic Dystrophy. (n.d.). https://rarediseases.org/rare-diseases/dystrophy-asphyxiating-thoracic/
[7] Orphanet: Jeune syndrome. (n.d.). https://www.orpha.net/en/disease/detail/474
[8] Schmidts, M., Arts, H. H., Bongers, E. M. H. F., Yap, Z., Oud, M. M., Antony, D., Duijkers, L., Emes, R. D., Stalker, J., Yntema, J. L., Plagnol, V., Hoischen, A., Gilissen, C., Forsythe, E., Lausch, E., Veltman, J. A., Roeleveld, N., Superti-Furga, A., Kutkowska-Kazmierczak, A., . . . Mitchison, H. M. (2013). Exome sequencing identifies DYNC2H1 mutations as a common cause of asphyxiating thoracic dystrophy (Jeune syndrome) without major polydactyly, renal or retinal involvement. Journal of Medical Genetics, 50(5), 309–323. https://doi.org/10.1136/jmedgenet-2012-101284
[9] Patel, A. (2015). Antenatal Diagnosis of Jeune Syndrome (Asphyxiating Thoracic Dysplasia) with Micromelia and Facial Dysmorphism on Second-Trimester Ultrasound. Polish Journal of Radiology, 80, 296–299. https://doi.org/10.12659/pjr.894188
[10] Stranks, L., Barry, S., & Yeo, A. (2021). A curious case of asphyxiating thoracic dystrophy in an adult. Respirology Case Reports, 9(12), e0876. https://doi.org/10.1002/rcr2.876