
Pectus carinatum, also known as “pigeon chest” or “keel chest,” is a type of chest wall deformity characterized by the protrusion of the sternum and ribs. Although it may be present at birth, it often becomes more noticeable during the rapid growth period of adolescence (puberty). The causes of pectus carinatum can be broadly classified into two categories: primary (congenital or idiopathic) and secondary (acquired).
What is Pectus Carinatum?

Pectus carinatum is a common anterior chest wall deformity, mainly characterized by the protrusion of the sternum, and it may also involve the ribs or costal cartilages.
In general, this convex deformity is not dangerous and does not affect life expectancy. Most individuals with pectus carinatum do not exhibit noticeable symptoms. However, in severe cases, patients may experience upper respiratory infections, shortness of breath, reduced exercise tolerance, and fatigue. It is worth noting that pectus carinatum can cause a noticeable change in chest appearance, which may lead to various psychological issues (e,g., low self-esteem or social anxiety). These psychological problems may, in turn, negatively affect physical health, leading to symptoms such as chest tightness or chest pain during certain activities or postures.
Some data suggest that approximately one in every 2,500 live births is affected by pectus carinatum, with a male-to-female ratio of about 4:1[1]. However, the actual incidence may vary significantly depending on the study population.
What Causes Pectus Carinatum?
The exact cause of pectus carinatum is not yet fully understood, and several theories currently exist.
1) Primary Pectus Carinatum (present at birth, not caused by another condition)
Pectus carinatum that is considered congenital or of unknown cause is generally classified as primary pectus carinatum.
In addition to cases with no clearly identified cause, research suggests that primary pectus carinatum may be associated with the following factors:
1. Congenital Developmental Abnormalities: During fetal development or early childhood, imbalanced growth of the sternum and costal cartilage may lead to protrusion of the sternum and ribs, resulting in pectus carinatum.
2. Genetic Factors and Family History: Pectus carinatum may be linked to genetic factors. Individuals with a family history of chest wall deformities are more likely to develop this condition. Studies suggest that a family history may be present in up to 33% of patients with pectus carinatum.
2) Secondary Pectus Carinatum (caused by an underlying disease or condition)
Secondary pectus carinatum may be associated with the following acquired causes:
1. Vitamin D or Calcium Deficiency (Rickets): One of the most commonly cited causes of pectus carinatum is Vitamin D or calcium deficiency. During growth and development, inadequate nutrition—especially insufficient intake of vitamin D and calcium—may lead to nutritional disorders such as pediatric rickets. In this condition, reduced bone hardness causes the anterior chest wall to protrude under continuous cardiac impact, eventually forming pectus carinatum.
2. Secondary to Thoracic Diseases: Some chest conditions, such as congenital heart disease and chronic respiratory infections, can cause abnormal development of the chest wall, eventually leading to pectus carinatum.
3. Secondary to Surgical Interventions: Certain surgical procedures may disrupt the integrity and stability of the chest wall structure, leading to pectus carinatum. A common example is heart surgery in young children.
4. Genetic Conditions Associated With Pectus Carinatum: Secondary pectus carinatum is often associated with some genetic disorders that affect connective tissue or skeletal development, leading to chest wall deformities, such as:
-
Marfan syndrome: A condition that impacts the body's connective tissue, commonly causing long limbs, heart problems, and chest deformities.
-
Noonan syndrome: A genetic disorder affecting normal growth, with typical features like unusual facial characteristics, short stature, and heart issues.
How Is Pectus Carinatum Diagnosed?
Diagnosis begins with a physical examination to gather key information about the chest deformity.
Routine tests typically include electrocardiogram (ECG) and chest X-ray.
CT scans may be considered if other associated conditions are suspected.
* Note: Wenlin Chest and Flat Pectus Carinatum are often misdiagnosed as pectus carinatum. However, they have more specific characteristics, and traditional pectus carinatum surgical techniques are not suitable for these conditions.
Further reading: 5 Commonly Misdiagnosed Chest Wall Deformities
Pectus Carinatum Treatment: Conservative and Surgical Techniques
The choice of pectus carinatum treatment depends heavily on the patient’s age and the preferences of the patient and their family.
1) Conservative Treatment (Non-Surgical)
Orthotic bracing is suitable for young children and adolescents with mild deformities. The child wears a custom pectus carinatum brace that applies pressure to the sternum to correct pectus carinatum. Additional supportive measures may include nutritional improvement, exercise therapy, and psychological counseling.
2) Surgical Treatment (Open or Minimally Invasive)
1. Open Surgery
Pectus carinatum has been surgically treated for many years, and early procedures often involved long incisions to correct the deformity.
One classic open surgical technique for pectus carinatum is the “sternal osteotomy,” also known as the “sternal depression procedure.” This technique involves performing a wedge osteotomy at the highest point of sternal protrusion, resecting or cutting the excessively long costal cartilages, then depressing the sternum to its normal position and fixing it tometal bars.
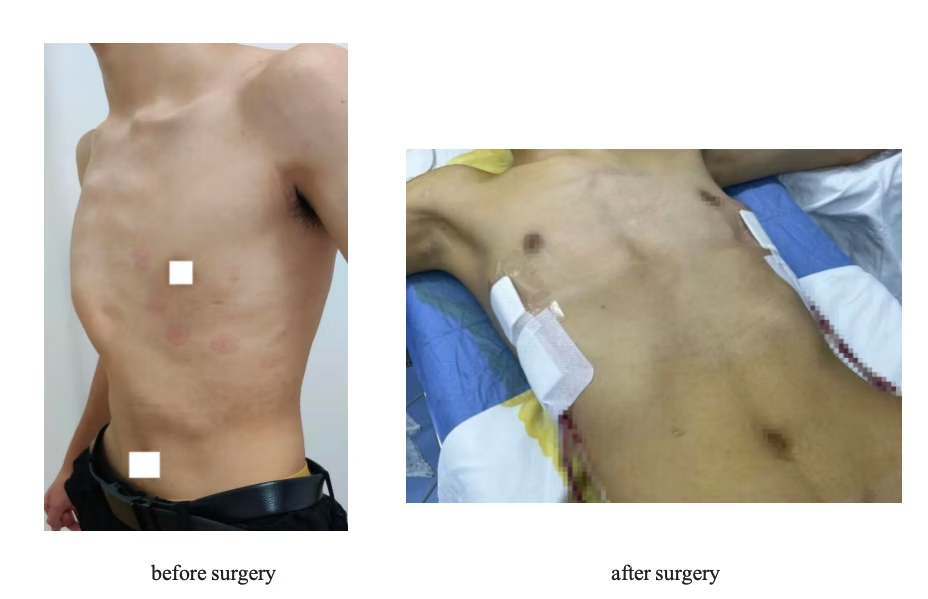
2. Minimally Invasive Surgery
In recent years, minimally invasive procedures for pectus carinatum have shown excellent outcomes. Compared with traditional open surgery, minimally invasive surgery offers smaller incisions, shorter operation times, fewer complications, and faster recovery.
-
Abramson procedure: A metal bar is used to compress the protruding chest wall and is then fixed to the ribs on both sides to achieve deformity correction. However, due to limitations of
inthe fixation method, the metal bar implanted is prone to displacement, adversely affecting the corrective outcome. -
Wenlin procedure: Pioneered by Dr. Wenlin Wang, the Wenlin procedure is an innovative surgical technique specifically for pectus carinatum. Compared with the Abramson procedure, it incorporates advanced surgical innovations, such as the “Wang Technique” for securing the bar and the “Pre-shaping” concept, which releases and reshapes protruding bony structures before the bar is applied. These approaches effectively avoid many of the risks and drawbacks of the Abramson procedure, offering smaller surgical trauma, better correction outcomes, greater safety and simplicity, shorter recovery time, and a lower complication rate.
Further reading: Pectus Carinatum Surgery: What You Need to Know
Contact ICWS for Professional Diagnosis and Treatment
ICWS specializes in advanced minimally invasive surgical techniques, including the Wenlin procedure, to correct chest wall deformities such as pectus carinatum.
The ICWS team has over 15 years of experience in chest wall disorders, covering a wide range of conditions such as chest wall deformities, trauma, tumors, defects, and infections, with a focus on personalized surgical planning, minimal trauma, and optimal cosmetic outcomes.
If you or your loved one is facing challenges from pectus carinatum, seeking professional evaluation is the next step. Feel free to contact ICWS anytime to discuss all treatment options, including whether minimally invasive surgery is suitable for your specific case.
Reference:
[1] Janssen, N., Coorens, N. A., Franssen, A. J. P. M., Daemen, J. H. T., Michels, I. L., Hulsewé, K. W. E., Vissers, Y. L. J., & De Loos, E. R. (2024). Pectus excavatum and carinatum: a narrative review of epidemiology, etiopathogenesis, clinical features, and classification. Journal of Thoracic Disease, 16(2), 1687–1701. https://doi.org/10.21037/jtd-23-957


